
The current Ebola outbreak in Democratic Republic of Congo (DRC) is the worst on record in the country and the second-largest epidemic of the disease recorded anywhere. Almost a year after the declaration of the outbreak, more than 2,190 people have died from the virus.
The Ebola crisis in DRC continues to pose a threat to local communities—despite a massive international response, promising new vaccines and treatments, and improvements in the medical management of the disease.
On July 17, 2019, the World Health Organization declared the Ebola outbreak in DRC a public health emergency of international concern.
Ebola is not the only public health emergency in DRC. The main causes of mortality in the country’s eastern region remain preventable diseases such as malaria and measles. In many health zones, only limited health care is available, as was the case even before the Ebola epidemic.
Many health workers have also now been recruited away from hospitals and health centers across the region by the internationally funded and well-paying Ebola response elsewhere. The staff shortages and a lack of financial resources and medical supplies for non-Ebola medical needs threatens to further weaken the health system and lower communities’ acceptance of the Ebola response.
A substantial amount of resources have been invested in the Ebola response since the beginning of the epidemic. Doctors Without Borders/Médecins Sans Frontières (MSF) strongly encourages actors and donors to consider the wider needs of the population rather than focusing response efforts on Ebola alone.
Ebola situation report as of November 15, 2019:
|
Total cases: 3,292 |
*Data reported by the DRC Ministry of Health and published by the World Health Organization.
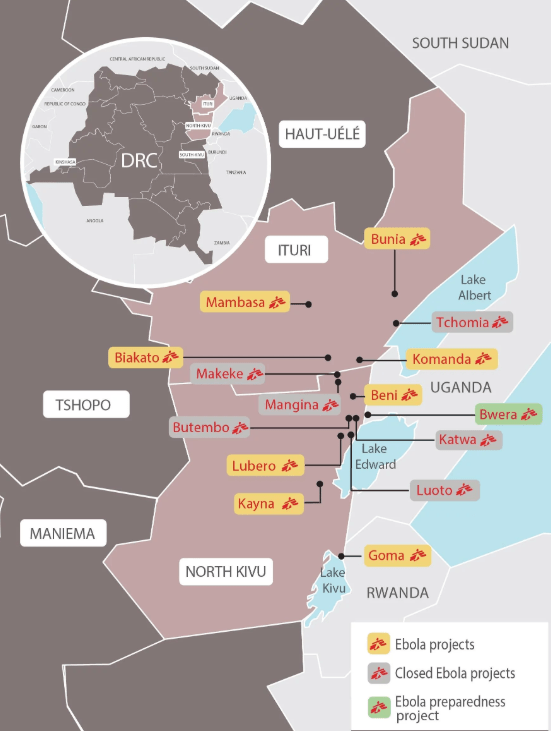
Cases of Ebola have been reported in North Kivu, Ituri, and South Kivu provinces, with the current hotspots located in Ituri province.
While the rate of transmission has appeared to slow down over the past month—averaging 47 new cases per week in September compared to August’s weekly average of 65 new cases—the overall fatality rate remains high. In total, 157 new Ebola cases were identified during the month of September, compared to 306 newly identified cases in August.
The Ministry of Health officially declared the outbreak on August 1, 2018, but it likely began months earlier. This is the tenth outbreak of Ebola in DRC in 40 years and by far the country's largest on record. It is also the second-largest Ebola epidemic ever in any country, behind only the West Africa outbreak of 2014–2016.
Ebola response
MSF is an active player in the Ebola response, caring for patients in four Ebola treatment centers (ETCs) in Bunia, Beni, Goma, and Mwenga, as well as numerous decentralized isolation and transit facilities where people with suspected cases of Ebola are tested before going to a treatment center if needed.
MSF also supports infection prevention and control (IPC) in local health care facilities and vaccination activities in the region. Our main priorities are assessing community health needs, providing timely health care to Ebola patients, ensuring appropriate IPC standards in health care facilities, and improving access to and quality of non-Ebola-related health care.
MSF projects follow an integrated approach, aiming to support health centers and hospitals, investing in primary and secondary health care together with Ebola-related activities. MSF does not have any projects that focus on Ebola alone.
Since early September, MSF has supported Ebola vaccination activities in Beni with three teams. Additionally, in several projects in the area, MSF supports routine and mass vaccination campaigns against measles, a primary health concern identified by communities in the region.
In total, 13 health zones in northeastern DRC have reported people who have Ebola in the last three weeks. While no new cases have been identified for two months in the city of Goma—the capital of North Kivu and a city of two million people located on the Rwandan border—the current hotspots are now shifting from North Kivu to Ituri province, with Mambasa, Komanda, and Mandima reporting more than 50 to 60 percent of all recent cases. Mambasa is currently the primary hotspot, and there are not enough beds at the moment to admit all people who are suspected or confirmed to have Ebola. Kalunguta is another North Kivu hotspot.
Key challenges
Ending the Ebola outbreak remains a complex endeavor. While fewer people have been confirmed to have Ebola in recent weeks, the epidemiological data show that further efforts are needed to improve the response. New Ebola patients are confirmed with an average delay of five days from the onset of symptoms to diagnosis—a time in which they are infectious to others and miss out on the benefits of receiving early treatment that would improve their chances of survival.
Only 25 percent of new Ebola cases in the outbreak—33 percent in the last two months—are identified and monitored as contacts of people previously confirmed to have Ebola. Two-thirds of direct and indirect contacts are lost or never followed-up with, risking further transmission.
The new treatments for confirmed Ebola patients available in ETCs are used under a study protocol framework that does not allow access beyond a particular patient or health worker. Extended use, like for additional protection for high-risk contacts, is not currently supported by the protocol. While confirmed patients and health workers benefit from the medication, their overall use remains restricted.
Persistent fear and misconceptions around Ebola treatment facilities and vaccination activities in local communities pose an additional challenge. One-third of all deaths have occurred in homes and communities where treatment was not available and people weren’t properly isolated to minimize the risk of spreading the disease.
Additionally, fighting between armed groups as well as targeted violence can limit crucial activities like vaccination, surveillance and contact tracing, community health promotion, and safe burials in some areas. While it is paramount that health care providers and their facilities are respected, it is equally as important that health care providers work to truly earn the trust of the communities they seek to serve.
Community engagement
Putting communities and patients first—and treating patients as people, not biological threats—is crucial to ending the epidemic. Community dialogue and engagement must form the cornerstone of the Ebola response.
For many communities across the affected region, the Ebola outbreak is only one of several pressing medical concerns. Of patients admitted to Ebola transit and treatment centers with symptoms like fever, vomiting, or diarrhea, only 4 percent have tested positive for Ebola, while the rest have other health needs.
For most of the epidemic, the response has too narrowly focused on fighting Ebola while other concerns have gone unheard and neglected. As a consequence, health and humanitarian workers risk losing the trust and acceptance of the very communities they are trying to serve.
Where communities ask for health care services for illnesses other than Ebola, their needs should be taken seriously and an appropriate response implemented alongside, or sometimes before, direct Ebola-response actions. Several MSF projects have adjusted their approach based on lessons learned since the outbreak began.
In all our Ebola emergency and regular projects in the region, MSF is committed to planning, implementing, and evaluating activities with input from the communities we serve. MSF projects start with an open community dialogue exploring needs and assessing what MSF can do to meet those needs. In Biakato, the community asked MSF first to build water points and support primary health care before asking for a transit center for suspect Ebola patients. In Beni, MSF decentralized isolation zones to local health centers bringing them closer to communities. All MSF ETCs and Ebola transit centers are supported by community outreach and health promotion activities, including messaging on the Ebola epidemic as well as other key health and hygiene information.
Vaccination
Over the past few weeks, preparations to introduce a new Ebola vaccine have been underway in two health districts in Goma. On November 13, DRC’s Ministry of Health announced that immunization with the second vaccine, Ad26.ZEBOV/MVA-BN-Filo—manufactured by Johnson & Johnson (J&J)—will begin as part of a large-scale clinical study in areas of the country affected by the ongoing Ebola epidemic. MSF is a partner in a consortium of international organizations involved in planning and implementing the study.
Approximately 23,000 doses of the Ad26.ZEBOV/MVA-BN-Filo vaccine have arrived in the country, meaning more people who are at risk of contracting Ebola can potentially be protected. Additionally, the study will result in more data on this second Ebola vaccine, which could pave the way for another approved tool to fight future Ebola epidemics.
Previously rVSV-ZEBOV, produced by Merck Pharmaceutical Corporation, was the only approved vaccine against Ebola. This vaccine is estimated to offer effective protection for 97.5 percent of participants ten days after vaccination and is a promising tool in the fight to contain the outbreak.
However, due to the limited use and investigational status of this vaccine, the vaccination strategy is limited to a “ring approach.” This means only contacts of people who likely or have been confirmed to have Ebola and their contacts—plus frontline workers like doctors and humanitarian staff who are most likely to interact with people who have Ebola—are eligible to be vaccinated.
The “ring vaccination approach” strongly depends on successful contact tracing, which has been notoriously difficult in DRC with an estimated 66 percent of contacts in the last three months not being followed, and 75 percent in the outbreak overall. MSF supports the Strategic Advisory Group of Experts’s (SAGE) recommendations to begin geographic vaccination, use pop-up sites, and expand vaccination activities.



